Patients with a debilitating hand condition are missing out on a simple treatment that
could spare them painful surgery, experts have warned.

Patients with the Iron Lady’s ‘claw hand syndrome’ are missing out on effective treatment because GPs are unaware of the options available.
- Margaret Thatcher suffered from Dupuytren’s contracture – known as claw hand
- Two million Britons suffer the condition which can be helped with radiotherapy
By Erin Dean
Published: January 13, 2024
Patients with a debilitating hand condition are missing out on a simple treatment that could spare them painful surgery, experts have warned. Blasts of radiotherapy, usually used to tackle cancer, can ease Dupuytren’s contracture – problems with hand tendons which lead to permanently bent fingers. But few hospitals offer it for the condition and many GPs are unaware it’s an option, say campaigners.
Two million Britons have some degree of Dupuytren’s, often called ‘claw hand’. Famous sufferers have included Margaret Thatcher and actor Bill Nighy. The cause is unknown but it runs in families and worsens with age, affecting about 20 per cent of over 65s.

a condition which affects an estimated two million Britons
Expert Non-Invasive Treatment for Dupuytren’s and Ledderhose Disease Across the UK
Dr Richard Shaffer set up Dupuytren’s UK in April 2011 to provide non-invasive treatments for people who suffer from benign conditions such as Ledderhose disease and early-stage Dupuytren’s contracture in the Guildford area. Today, Dupuytren’s UK offers this service to patients throughout the UK.

According to charity The British Dupuytren’s Society, the standard approach is to wait until the condition is severe, causing the fingers to bend completely inward, before offering straightening surgery. The op involves cutting away parts of the affected
tendons or removing them completely.
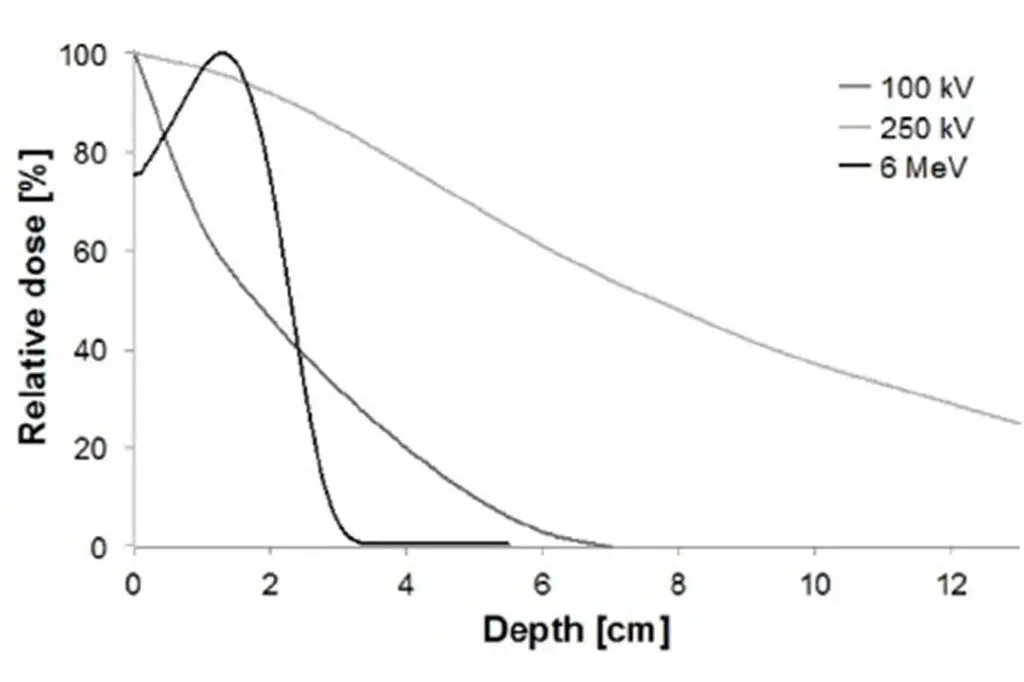
A third of patients need more than one op and some may even need to have fingers amputated. But radiotherapy, offered earlier on, may prevent patients from needing to go under the knife. It is provided in ten sessions of a minute each and at a much lower dose than for cancer care. It works by breaking down the tough bands and lumps that form in the hand tendons – the cause of the contracture.
Anna Schurer, chairwoman of the British Dupuytren’s Society, says: ‘Radiotherapy is the only treatment that offers hope of preventing Dupuytren’s from worsening. ‘Before the pandemic we knew of many hospitals that provided the treatment, but this list has now dwindled to four in England and one in Scotland on the NHS.’
Dr John Glees, a private consultant clinical oncologist, provides radiotherapy for Dupuytren’s and says it can improve the condition for patients with early disease.
In an audit of more than 150 patients treated between 2010 and 2015, Dr Glees, who sees patients at the Nuffield Health Cancer Centre London in Wimbledon, found that there was complete resolution or major improvement in 60 per cent of cases, minor
improvement in 22 per cent and just 13 per cent did not improve.
‘It is so frustrating that more people cannot access this treatment on the NHS,’ he says. ‘It is such a common condition, but patients go to their GP and get told to come back when it is much worse, and surgery results are often poor.’
Dr Richard Shaffer, a consultant clinical oncologist at the Cromwell Hospital in London, uses radiotherapy to treat about 400 patients with Dupuytren’s each year. The private treatment costs about £3,000. He says: ‘The evidence suggests it is a highly effective preventative treatment that reduces the risk of getting a contracture [when the fingers become completely bent inward] and needing surgery.
But NHS provision is patchy, there are capacity issues in terms of the radiotherapy machines and staffing to provide this care, when it is also needed for cancer patients. But it is a concern that it is not more available.’

Dr Stephen Falk, a consultant clinical oncologist at University Hospitals Bristol NHS Foundation Trust, adds: ‘I think radiotherapy centres are anxious that if they open the floodgates to benign disease [such as Dupuytren’s] they would be swamped.’
He says a key stumbling block was a 2016 decision by NHS watchdog the National Institute for Health and Care Excellence not to back radiotherapy for Dupuytren’s.
It recommended that it could be offered only under ‘special arrangement’, meaning there are uncertainties around how effective or safe a treatment is, and requires doctors offering it to collect data on outcomes.
Part of the concern was a theoretical risk of radiation-induced cancer, which meant that NHS bosses stopped funding the treatment in some areas.
However, the Royal College of Radiologists, in guidance updated last March, reviewed the most recent research and recommended it as a treatment for Dupuytren’s.
A lack of knowledge among doctors about the existence of early treatment options is also a problem. ‘Patients can’t get referred even in areas where it is offered on the NHS, as GPs don’t know about it,’ Ms Schurer says.
One happy patient is Barry Williams, 77, a retired lawyer, who says radiotherapy completely solved his early Dupuytren’s, allowing him to keep playing the piano.
Barry says he had been alert for signs of the condition after seeing his father and grandmother suffer from the problem.
‘My father had many awful operations, eventually having his left little finger amputated,’ he says.
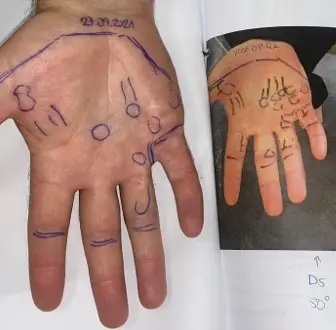
Barry had private treatment with Dr Glees more than a decade ago when he spotted early signs of the disease. At the time his only symptom was puckering in on his palms, which occurs as the build-up of tissue starts to form beneath the skin, pulling
it down.
‘The treatment was painless, I had no side effects and I have had no problems in the 14 years since,’ says Barry.
‘Without this I would have been completely disabled, my hands would be useless and I would be unable to play the piano.’