Ledderhose disease (plantar fibromatosis) causes firm lumps in the sole of the foot that can become painful and interfere with walking. This guide explains why nodules form, what happens over time, and compares all treatment options — from footwear changes and injections to surgery and radiotherapy — with a clear, evidence-based focus on what works best.


What Is Ledderhose Disease?
Ledderhose disease, also called plantar fibromatosis, is a condition where firm lumps develop in the sole of the foot. A single lump is called a plantar fibroma.
Many people describe it as “Dupuytren’s disease of the foot,” and that is a helpful way to understand it. It belongs to the same group of conditions where the body produces too much scar tissue. In the hands, this causes Dupuytren’s disease. On the knuckles, it causes Garrod’s pads. In the penis (Peyronie’s disease), it causes curvature. In the feet, it causes nodules in the arch or under the ball of the foot (Ledderhose disease).
Under the microscope, the tissue looks the same as Dupuytren’s disease. It is essentially scar tissue that has grown more than it should.
The nodules most commonly appear in the arch of the foot. Toe contractures are rare. The reason is probably mechanical. We walk with our toes extended and the fascia stretched, which makes shortening far less likely than in the hand.
For most people, the main issue is pain and tenderness. Sometimes the bulkiness of the lump also makes certain shoes difficult to wear.
Why Do Some Nodules Hurt and Others Don’t?
Not all nodules behave the same way. Whether they cause pain depends on several things: where they sit in the foot, the shape of your arch, whether you are stepping directly on them, and whether the lump has only recently appeared or has been there for a long time.
A lump that sits under the ball of the foot, or further back towards the heel, may be stepped on repeatedly and become painful quite quickly, whereas a lump that sits high in the middle of the arch may not be pressed on very much.
When nodules first appear, they are often tender. Over time, some settle down by themselves. Around one in five may become less painful or shrink spontaneously without treatment.
Size alone does not predict pain. I have seen very small nodules that are very sore, and larger ones that cause little discomfort. And actually response to treatment does not clearly depend on size either.
What Usually Happens Over Time?
If someone comes to see me very early, I usually make sure the lump has been present for at least a few months before considering treatment. Some nodules improve or settle by themselves, and there is no benefit in rushing into treatment unnecessarily.
At the other end of the spectrum, disease can become quite bulky and widespread. I recently treated a patient who had nodules under the ball of her foot which had become so large that they were lifting her toes off the ground. She described her pain as 8 or 9 out of 10 (on a scale where 0 means no pain at all and 10 means the worst pain imaginable). After one week of radiotherapy, her pain fell to zero.
Pain can also change the way someone walks. People naturally try to avoid stepping on a sore area, and that can lead to discomfort elsewhere in the foot or in the Achilles tendon.
Treatment Options
Treatment falls into five broad categories:
- Conservative measures
- Medications and injections
- Shockwave therapy
- Surgery
- Radiotherapy
Conservative Measures
Conservative treatment is always the first step and is often very effective.
Good footwear makes a real difference. Well-cushioned shoes with supportive soles can reduce pressure on the nodules. Thin-soled or unsupportive shoes often make symptoms worse. Many people find that walking barefoot on hard floors, rocky beaches, or uneven ground increases their pain.
Standard arch-support insoles can sometimes worsen symptoms because they press directly into the arch where the nodules sit. Some patients cut a hole in the insole so that the lump can sit inside it without being pressed on. This works best when there are only one or two protruding nodules. Custom insoles can also help, although nodules may grow or shrink over time, which can limit how well a fixed device continues to fit.
For mild cases, simple changes to footwear and activity can be enough to control symptoms.
Expert Non-Invasive Treatment for Dupuytren’s and Ledderhose Disease Across the UK
Dr Richard Shaffer set up Dupuytren’s UK in April 2011 to provide non-invasive treatments for people who suffer from benign conditions such as Ledderhose disease and early-stage Dupuytren’s contracture in the Guildford area. Today, Dupuytren’s UK offers this service to patients throughout the UK.

Painkillers
Simple painkillers can sometimes take the edge off discomfort, but they are rarely a complete solution. Painkillers can also have significant side effects. For instance, codeine can cause constipation and drowsiness, and anti-inflammatory medicines such as ibuprofen can irritate the stomach or affect kidney function. They may provide temporary relief, but they do not address the underlying condition.
Creams and Injections
Verapamil cream is sometimes prescribed and has to be specially prepared in a compounding pharmacy. There is no evidence in the medical literature supporting its use in Ledderhose disease, although some patients report benefit.
Steroid injections are sometimes used and may provide temporary pain relief. For some people they help for a short period; for others they are uncomfortable and the benefit does not last. They do not reliably prevent the nodules from growing further.
Hyaluronidase (enzyme) injections are promoted by some clinicians, particularly in the United States, with claims of dramatic shrinkage and pain relief. At present, however, there is no strong published evidence supporting their use in Ledderhose disease.
Shockwave Therapy
Shockwave therapy uses sound waves delivered into the tissue. It is commonly used for conditions such as plantar fasciitis.
There is some early evidence suggesting it may reduce pain in Ledderhose disease, but the studies are small and the long-term effects are uncertain. Ledderhose disease occurs because the body produces too much scar tissue. Shockwave therapy stimulates tissue repair. There is therefore a theoretical risk that while it might reduce pain initially, it could encourage further growth of the nodules over time. For that reason, I remain cautious about its use.
Surgery
Surgery is sometimes offered, particularly when nodules are large. The simplest operation removes the lump itself. In around 80% of cases, the nodules grow back. Often they return more aggressively, and the scar tissue from surgery can itself be painful and thickened.
A more extensive operation (called a total plantar fasciectomy) removes the whole plantar fascia. This is a major procedure with a long recovery period and a significant risk of wound problems. It should only be considered as a last resort, and certainly not before radiotherapy has been tried.
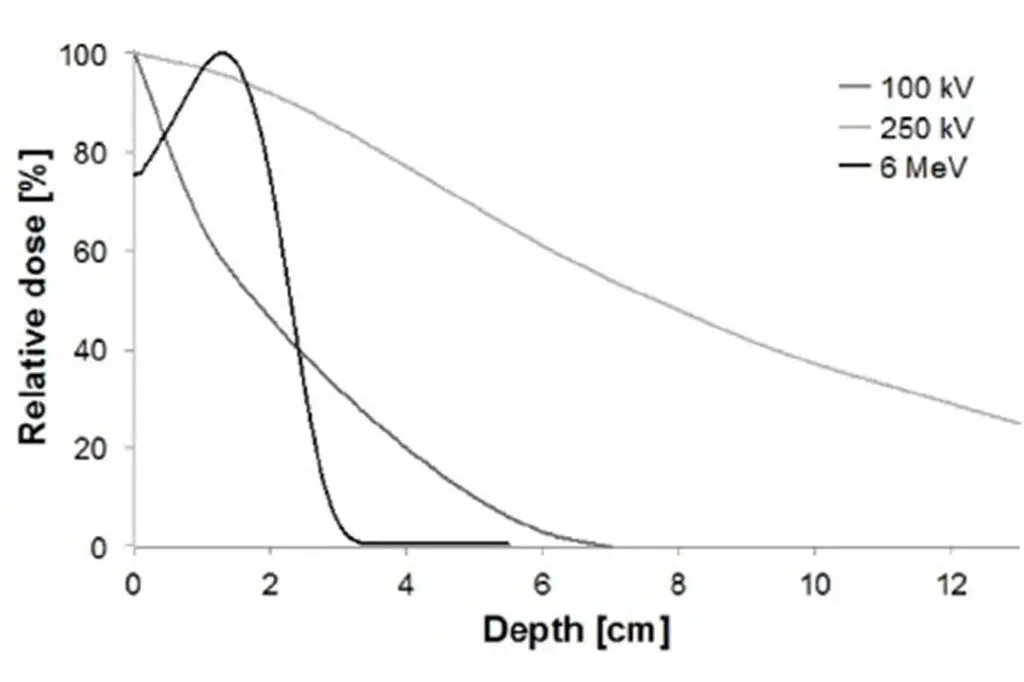
Radiotherapy
Radiotherapy has the strongest evidence behind it of all the active treatments for Ledderhose disease. Studies from Germany have shown that around 70-80% of patients experience meaningful improvement in pain and stabilisation of the disease over five years.
In 2023, a high-quality trial from the Netherlands compared real radiotherapy with a sham (placebo) treatment. All patients were set up on the machine in exactly the same way, but some received real radiation and others did not. At six months, both groups improved somewhat, which is common in pain conditions. By twelve months, however, the difference was clear. The group that received the real radiotherapy treatment had significantly better pain reduction, better function, and better quality of life.
Radiotherapy reduces pain, reduces the size of the nodules, and stops them from growing further. It’s important to know that it sometimes works quite slowly. I always tell patients to judge the result at around one year after the end of the treatment. Some people may even have further gradual improvement at eighteen months or even two years.
Because it takes time to reach its full effect, it makes sense not to wait until the pain becomes severe before seeking treatment. If you wait until the condition is agonising, you may spend a year in significant discomfort while waiting for improvement.
Bringing It Together
After you have tried sensible footwear adjustments and activity changes, radiotherapy is the most evidence-supported treatment for Ledderhose disease. Other injections and shockwave treatments lack strong evidence and may carry risks. Surgery has a high chance of the nodules growing back and can leave painful scar tissue.
Radiotherapy has been shown in proper clinical trials to reduce pain and improve quality of life. I have found it very rewarding to treat patients who come in struggling even to walk comfortably and then, over time, see them return to normal daily activities – walking, travelling, exercising – without pain. Most patients do respond and regain a completely normal quality of life.
That, ultimately, is the goal: to restore comfort, mobility, and the ability to stand, walk and run normally again.