If you’ve been told that nothing can be done for Dupuytren’s disease until your fingers are bent, you’re not alone. This guide explains why this advice is common in the NHS, what it actually means, and how to explore early assessment and treatment options.


If you’ve been told that nothing can be done for your Dupuytren’s disease until your fingers are bent, you’re not alone. This is one of the most common things patients are told, either by their GP or sometimes by a specialist.
At the same time, many people have looked online or on social media and seen quite severe cases, where the fingers are very bent and surgery has been needed. Seeing that can be unsettling, particularly if you’ve just noticed a lump or some tightening in your hand.
So you end up in an uncomfortable position. You’re being told to do nothing, but you can see what might happen if the condition progresses. It’s not surprising that this creates uncertainty.
What “nothing can be done” usually means
When a GP or specialist says that nothing can be done, it usually reflects what is available within the NHS at that stage of the condition.
The NHS pathway for Dupuytren’s disease is mainly focused on more advanced disease. In practice, this often means either being advised to wait and see, or being referred to a hand surgeon once a contracture has developed and is affecting function.
That approach is based around surgery, which is designed to correct a bent finger once it has developed. Because of that, earlier stages of the condition are often not actively treated within that system.
Why this doesn’t always feel right to patients
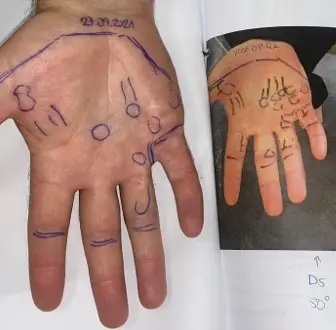
For many people, this approach doesn’t sit comfortably. You may be able to feel nodules in the palm, notice tightness, or feel that your fingers are not moving quite as freely as before.
Even if these changes are still relatively mild, they are noticeable. Waiting for the condition to become more advanced before doing anything about it doesn’t feel like a good strategy, particularly if you rely on your hands for work, sport, or everyday activities.
There is also the added factor of seeing more severe cases online, which can make it feel as though you are being asked to wait for something that you would rather avoid.
Expert Non-Invasive Treatment for Dupuytren’s and Ledderhose Disease Across the UK
Dr Richard Shaffer set up Dupuytren’s UK in April 2011 to provide non-invasive treatments for people who suffer from benign conditions such as Ledderhose disease and early-stage Dupuytren’s contracture in the Guildford area. Today, Dupuytren’s UK offers this service to patients throughout the UK.

Taking a more proactive approach
An alternative to simply waiting is to take a more proactive approach and have your condition properly assessed at an earlier stage.
This doesn’t mean committing to treatment. It means understanding where you are in the course of the disease and what your options are, so that you can make a decision based on your own situation.
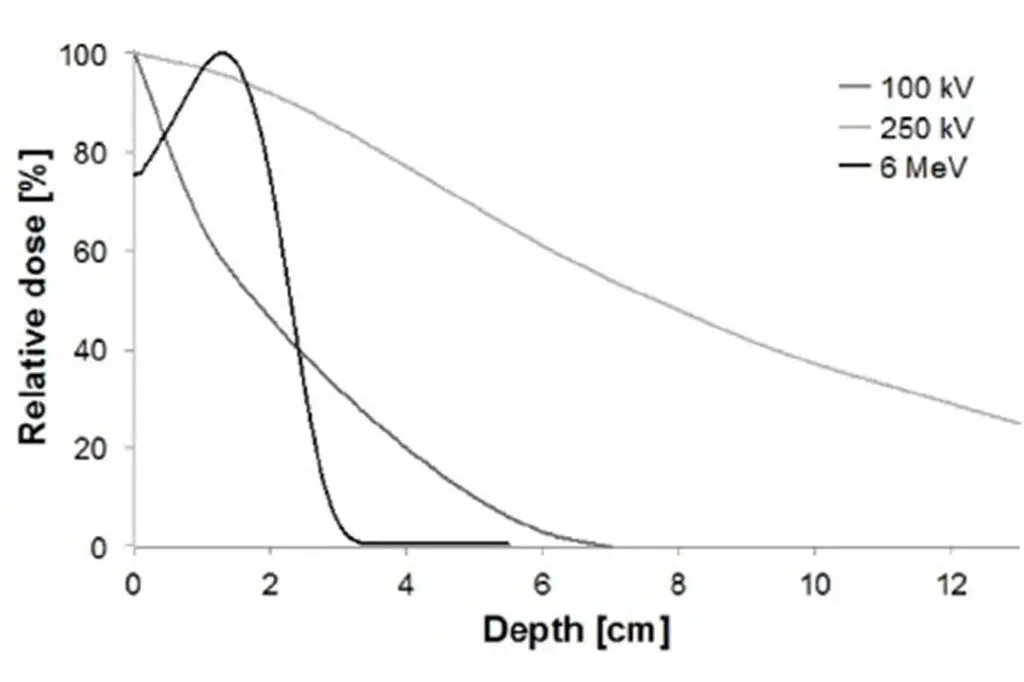
Radiotherapy is one of the options that can be considered in early, active Dupuytren’s disease. It is used when there are nodules or early tightening and where the condition is changing over time or beginning to affect function in a minor way.
The aim of radiotherapy is to stabilise the condition and reduce the chance of progression and the need for surgery. It is not designed to reverse a bent finger once a contracture has developed.
Why timing matters
One of the key differences between early and late disease is that the treatment options are different.
Radiotherapy is most effective when the disease is still at an early stage. Once a more significant contracture has developed, it is no longer effective, and the focus shifts to procedures that release the tight tissue, such as needling or surgery.
This is why relying solely on a “wait and see” approach can be frustrating for some patients, as it may mean missing the stage where preventative treatment is possible.
What happens when you are assessed early
Seeing a doctor who specialises in treating patients with early Dupuytren’s disease allows you to understand where you are in that pathway.
If the disease is very early and stable, you may simply be advised what to look out for and how to monitor it over time.
If it is more advanced, you can be referred to a surgeon for further assessment.
If it is early but clearly progressing or beginning to affect function, then radiotherapy may be an option to help prevent further progression.
What to do next
If you have been told that nothing can be done, it is worth understanding that this usually reflects the NHS pathway rather than the absence of all treatment options.
The next step is to have your condition assessed so that you can understand your stage of disease and what options are available to you. This does not commit you to treatment, but it does allow you to make a decision based on clear, personalised information.
For many patients, that alone makes the situation feel much more manageable, as it replaces uncertainty with a clear plan of what to do next.