This is something I get asked by patients who had radiotherapy years ago and are now noticing new nodules or cords.


The short answer is: sometimes, yes. But the answer depends very much on what exactly is happening now, how well the first treatment was tolerated, and whether there is still active disease that radiotherapy is likely to help.
This is an area that causes a lot of confusion because people often hear very different opinions. Part of the reason is that there is very little published research specifically looking at repeat radiotherapy for Dupuytren’s disease.
What radiotherapy is trying to achieve
Radiotherapy for early Dupuytren’s disease is not designed to straighten severely bent fingers. Instead, the aim is to slow down or stabilise active early disease before major contracture develops.
Typically, treatment is considered when people notice progression over the previous months. That may mean enlarging nodules, the formation of new nodules, thickening cords, increasing tightness, or gradual loss of finger extension.
Most people who respond to radiotherapy remain stable long-term. However, Dupuytren’s disease is a condition that can remain active over many years, and some people therefore notice new growth later on, even after initially successful treatment.
It is also important to understand that the first year after radiotherapy can sometimes be a little unpredictable. Nodules may temporarily enlarge, soften, shrink again, or fluctuate before eventually stabilising.
That is one reason why I generally would not rush into repeat treatment very quickly after the original course. Early changes do not necessarily mean that the treatment has failed.
The three main situations
1. New disease in an area that was not previously treated
This is the simplest situation.
For example, somebody may later develop Dupuytren’s disease in the other hand, elsewhere in the same palm, or in the feet with Ledderhose disease. In these situations, the new area itself has not previously received radiotherapy.
That means the area can often be approached in the normal way that we would treat somebody having radiotherapy for the first time.
2. The original treatment never really seemed to work
Very unusually, some patients feel that the nodules simply continued progressing straight through treatment or immediately afterwards.
In that situation, repeating radiotherapy to exactly the same area is generally less likely to be effective. However, this still needs to be interpreted carefully, because nodules can fluctuate during the first year after treatment before eventually stabilising.
3. The treatment worked initially, but new activity developed years later
This is probably the commonest situation where repeat treatment is considered.
Typically, these patients had a good initial response, remained stable for years, and then later noticed new or enlarging nodules developing within or close to the original treated area.
In my own practice, if there are genuinely new or enlarging nodules, sometimes with a little associated tightness, then I will often consider repeat treatment.
On the other hand, if the main issue is worsening tightness without obvious new or enlarging nodules, then radiotherapy is often less likely to add very much. At that stage, the problem may relate more to the tightening of already established scar tissue than to ongoing biologically active disease.
Noticed changes since your last treatment?
If you had radiotherapy in the past and have new nodules, cords or tightness, it is worth having the area assessed properly before deciding what to do next. Get in touch with Dr Shaffer to arrange an assessment and talk through whether further treatment might help.

How repeat treatment is usually approached
For a first course of radiotherapy, many centres – including my own practice – often use relatively broad treatment fields covering most of the area at risk within the palm. However, there is considerable variation internationally. I have seen very small fields used, but also overly large fields.
Very small fields may potentially miss nearby areas where Dupuytren’s disease is already developing. Conversely, very large fields may include areas where Dupuytren’s disease does not normally form, unnecessarily increasing radiation exposure to normal tissue.
When I consider repeat treatment years later, my practice is usually different from the original wide-field approach. Rather than broadly treating most of the palm again, I would usually use a much smaller, focused field directed at the newly active area itself.
That usually means treating the new or growing nodules, sometimes including the nearby cord, plus a margin. The aim is to focus on the area of active progression while limiting unnecessary retreatment of unaffected tissues.
Is repeat treatment safe?
Overall, my own experience has been that repeat treatment is generally well tolerated when used carefully and selectively. In practice, I have not found that patients typically experience worse side effects than they did with the first course.
The key is patient selection and keeping the retreatment field relatively focused. The aim is not to re-irradiate large areas unnecessarily, but instead to concentrate on clearly newly active disease.
It is also important to understand that there is a limit to how much radiotherapy can safely be given to one area of the body over a lifetime. In simple terms, I explain this to patients as each area having an approximate maximum allowance of three “weeks” of Dupuytren’s radiotherapy treatment.
For the initial treatment, we normally use the standard full treatment course, which is delivered over two treatment weeks separated by a gap. If we later decide to retreat to the same area, I would usually use only a single further treatment week, rather than repeating the entire original course.
That means retreatment is not something that can simply be repeated indefinitely. We therefore have to think carefully not only about whether retreatment is appropriate, but also about the timing of retreatment and whether the current disease activity is significant enough that radiotherapy is genuinely likely to help.
Good decision-making, therefore, depends on having as much information as possible about the original treatment. The previous dose, treatment fields, overlap with the new area, previous response, and current pattern of progression all help guide whether further radiotherapy is sensible.
Is there good scientific evidence?
Not really, and I think it is important to say that openly.
There is good evidence supporting radiotherapy for early active Dupuytren’s disease in general. However, there is very little published evidence specifically looking at repeat irradiation of the same area.
That means these decisions are usually made on an individual basis using radiotherapy principles, clinical judgement, previous response, and an assessment of whether there is still active disease that radiotherapy is likely to help.
What should you do if new nodules appear years later?
The first thing is not to panic. New nodules do not automatically mean that the original treatment “failed”.
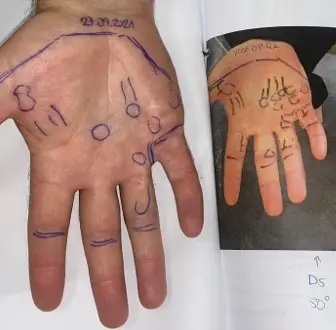
I often see patients in the clinic who notice a single new nodule a couple of years after radiotherapy. In many cases, when I compare the current hand with the original pre-treatment photographs, the overall situation still looks much better than before treatment.
In that situation, I will often simply document the area carefully, take updated photographs, and continue observing. A single small nodule without a new cord extending further into the finger may remain stable for years and may never become clinically important.
That is very different from somebody developing a new nodule together with a cord extending further into the finger, particularly if the finger is beginning to lose the ability to fully straighten. In that situation, I would lean much more strongly towards considering further treatment rather than continued observation alone.
If I treated you originally, I will already have access to your previous treatment plans, field arrangements, and photographs, which helps enormously when comparing the current situation with the original disease.
If your previous radiotherapy was given elsewhere, then it is very helpful to obtain details of the original treatment if possible. Previous clinic letters, treatment summaries, field diagrams, or radiotherapy doses can all help when deciding whether further treatment may be appropriate.
The bottom line
Yes, some patients can have radiotherapy more than once for Dupuytren’s disease. In selected situations, repeat treatment can be a reasonable option and is often well tolerated.
The most important issue is whether there is genuinely active progressive disease, particularly new or enlarging nodules or cords, rather than tightening alone without obvious new active disease.
If you have had radiotherapy in the past and are now noticing changes in your Dupuytren’s disease, please get in touch for an assessment.