If you have recently been diagnosed with Dupuytren’s disease, or you have found a lump in your palm and are trying to work out what to do next, one of the first questions is often surprisingly simple: which doctor should I actually see?


Many patients assume the answer is automatically a hand surgeon. In reality, it depends very heavily on the stage of the disease and what you are trying to achieve.
For people with advanced Dupuytren’s disease and significant finger contracture, hand surgeons are the experts. But for people with early Dupuytren’s disease, where the fingers are still straight or only mildly tight, the situation is different. In that setting, a radiation oncologist who specialises in early Dupuytren’s disease may actually provide a much more detailed assessment and a more appropriate management plan.
This article explains the difference between early and advanced Dupuytren’s disease, what each specialist typically focuses on, and why the type of doctor you see can significantly affect the advice you receive.
What is Dupuytren’s disease?
Dupuytren’s disease is a condition affecting the connective tissue underneath the skin of the palm. Over time, the tissue can thicken and form nodules and cords.
In some people, the disease remains mild and stable for many years. In others, it progresses and gradually pulls the fingers into a bent position called a contracture.
The ring and little fingers are most commonly affected, although any finger or the thumb can become involved. Some patients also develop related conditions such as Ledderhose disease in the feet or knuckle pads over the backs of the fingers.
What is the difference between early and advanced Dupuytren’s disease?
This distinction is extremely important because different stages of the disease are managed in different ways.
Early Dupuytren’s disease usually means that the fingers are still completely straight, or there is only mild tightening. Patients may notice:
- Small nodules in the palm
- Early cords beneath the skin
- Tightness or pulling sensations
- Tenderness or itching
- Mild loss of finger flexibility
- Early difficulty fully stretching the fingers backwards
At this stage, many patients still have excellent hand function.
Advanced Dupuytren’s disease is different. This is when significant contracture has developed and the fingers are clearly bent. Patients may struggle to put their hand flat on a table, place their hand in a pocket, wear gloves, shake hands comfortably, or grip larger objects.
This later stage is where surgical and needle-based procedures become much more important.
Why the doctor you see matters
One of the biggest frustrations patients describe is that they feel they receive very different advice depending on which specialist they see.
That is not necessarily because one doctor is right and another is wrong. It is often because surgeons and radiation oncologists are looking at different stages of the disease and treating different patient groups every day.
Hand surgeons are experts in correcting established contracture.
Radiation oncologists who specialise in Dupuytren’s disease are experts in assessing early disease progression and deciding whether early radiotherapy may help stabilise the condition before major contracture develops.
Those are not the same skill sets.
Getting the diagnosis right
The first job of any doctor is to confirm whether you actually have Dupuytren’s disease.
In most cases, the diagnosis is clinical. An experienced doctor can usually recognise Dupuytren’s disease simply by examining the hand.
This means that both experienced hand surgeons and experienced radiation oncologists are generally very capable of diagnosing typical Dupuytren’s disease.
Only occasionally is an ultrasound scan needed to clarify uncertainty.
There is sometimes an assumption that only surgeons can confidently distinguish Dupuytren’s disease from other hand conditions. In practice, experienced radiation oncologists who regularly see Dupuytren’s patients also become very familiar with alternative diagnoses.
For example, trigger finger, ganglion cysts, tendon problems, and other soft tissue lumps often have completely different examination findings.
Sometimes patients attend expecting radiotherapy, only to discover they do not actually have Dupuytren’s disease at all. That can be extremely reassuring for them.
What often happens at a surgical consultation
Most surgeons primarily treat advanced Dupuytren’s disease. Their clinics are naturally focused on patients whose fingers are already bent enough to require intervention.
As a result, many patients with early disease describe a fairly brief consultation. Typically, the surgeon examines the hand, confirms the diagnosis, and advises the patient to return once the fingers bend further.
From a surgical perspective, that approach is understandable. Surgery is generally not performed for small nodules with straight fingers.
However, many patients come away feeling that something is missing. They are often left wondering:
- How do I know if this is progressing?
- What exactly should I monitor?
- Am I already within the window where radiotherapy might help?
- How quickly is this changing?
- What activities should I avoid?
- When should I seek reassessment?
Those questions are central to early Dupuytren’s management.
What a radiation oncologist specialising in early Dupuytren’s disease does differently
A specialist radiation oncologist generally approaches early Dupuytren’s disease in a much more detailed way.
The aim is not simply to confirm the diagnosis. The aim is to determine whether the disease appears biologically active, whether treatment may be beneficial, or whether careful observation is more appropriate.
That requires a much more structured assessment.
During my own consultations, I do not simply feel the palm briefly and stop there.
I assess the entire pattern of disease carefully. That includes looking for nodules and cords in the palm, assessing the fingers individually, examining the thumb web space, and measuring flexibility in every affected digit.
I also routinely examine the feet for Ledderhose disease and look for knuckle pads, because these features help build a complete picture of the disease behaviour.
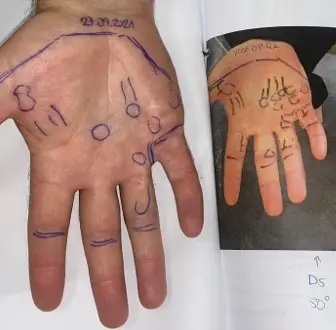
Importantly, I map and document every visible and palpable area of disease. This creates an objective baseline that can later be compared against future photographs and examinations.
Why monitoring matters properly
One of the biggest gaps in early Dupuytren’s management is that patients are often told to “watch and wait” without being told what they should actually be watching for.
Good observation is not passive.
A structured observation programme involves monitoring four main areas.
The first is the physical extent of the disease itself. Are there new nodules? Are cords becoming more obvious? Is the disease spreading into the fingers or the thumb web space?
The second is symptoms. Increasing tightness, tenderness, itching, aching, or pulling sensations can all suggest disease activity.
The third is finger flexibility. One of the earliest changes is often loss of hyperextension, meaning the finger gradually loses the ability to fully straighten backwards, even before obvious contracture develops.
The fourth is span. Changes in finger span or thumb span can indicate progressive tightening before patients notice major bending.
Without this sort of baseline assessment, many patients struggle to judge whether their disease is truly changing.
Not sure where your Dupuytren’s stands?
If you have early nodules, cords or tightness and want to understand whether your disease is active, a detailed specialist assessment can help. Get in touch with Dr Shaffer to talk through monitoring and whether early treatment might be right for you.

Deciding whether radiotherapy is appropriate
Another major difference is familiarity with early radiotherapy itself.
A surgeon may have views about radiotherapy, but they are usually not immersed in the detailed evidence surrounding early Dupuytren’s disease progression, patient selection, and long-term outcomes.
Radiation oncologists specialising in this area spend much of their time assessing exactly which patients are most likely to benefit and which are unlikely to need treatment.
That distinction matters enormously because not everybody with Dupuytren’s disease should automatically receive radiotherapy.
Some patients have tiny stable nodules that may never progress significantly. Others already show multiple signs of active disease despite having relatively straight fingers.
Those are very different situations.
Importantly, a responsible radiation oncologist should also be comfortable advising against treatment when appropriate.
In fact, many patients attending specialist early Dupuytren’s clinics are ultimately advised to continue observation rather than proceed immediately to radiotherapy.
Advice about activities and hand protection
Another area where specialist early Dupuytren’s clinics often differ is practical advice about activities and hand loading.
Many patients want to know whether certain activities might aggravate their disease.
Although Dupuytren’s disease is strongly influenced by genetics, repeated trauma and mechanical stress may still contribute to progression in some individuals.
This can include:
- Repeated blunt trauma to the palm
- Vibrational exposure
- Heavy gripping activities
- High tendon loading
- Impact through the palm
- Activities such as climbing or heavy manual work
The advice should not be generic or alarmist. It should be individualised. The goal is usually not to stop people from living their lives, but to help them understand sensible modifications that may reduce repeated stress on vulnerable tissue.
When a surgeon is absolutely the right person
None of this means surgeons are unimportant in Dupuytren’s disease. Far from it.
Once significant contracture develops, surgeons become central to management.
Patients with advanced disease may require:
- Needle fasciotomy
- Limited fasciectomy
- Dermofasciectomy
- Other corrective procedures
These treatments fall squarely within surgical expertise.
Similarly, if I see a patient whose disease is already too advanced for meaningful radiotherapy benefit, I will refer them to a trusted hand surgeon rather than simply suggesting observation.
Good Dupuytren’s care should not be about territorial disputes between specialties. It should be about matching the right patient to the right treatment at the right stage of disease.
So who should you see?
If your fingers are already significantly bent, a hand surgeon is usually the correct specialist to see.
If you have early Dupuytren’s disease with nodules, cords, tightness, or mild early contracture, then seeing a radiation oncologist who specialises in Dupuytren’s disease may give you a much more detailed assessment of progression risk, monitoring, and whether early radiotherapy is appropriate.
The key point is that early Dupuytren’s disease is not simply “nothing until surgery”.
There is a whole middle ground involving careful assessment, structured monitoring, activity advice, and consideration of early intervention in selected patients.
That is the area where specialist early Dupuytren’s radiotherapy clinics can provide significant value.
Final thoughts
Many patients with early Dupuytren’s disease feel caught between two extremes: either being told not to worry at all or waiting until the disease becomes severe enough for surgery.
In reality, early Dupuytren’s disease often deserves a much more nuanced assessment than that.
An experienced radiation oncologist specialising in Dupuytren’s disease can usually provide a detailed evaluation of disease activity, progression risk, monitoring strategies, lifestyle considerations, and whether radiotherapy may genuinely be helpful.
At the same time, good specialist care also means recognising when treatment is not needed, and when surgical referral is more appropriate.