Is it too early or too late for Dupuytren’s radiotherapy? Dr Richard Shaffer explains the timing window, the signs that matter, and when to get assessed.


One of the most common questions people ask after being diagnosed with Dupuytren’s disease is whether they are already at the right stage for treatment. Some people say, “My fingers aren’t bending yet, and it’s not affecting my hand function. Surely it’s too early?” Others worry they may already have left things too late, and ask whether radiotherapy can still help once the fingers have become noticeably bent.
Both concerns are understandable. Dupuytren’s disease often develops slowly over years, and many patients are trying to work out whether they should simply monitor things, consider radiotherapy, or start thinking about surgery. The difficulty is that “early Dupuytren’s disease” covers a very wide spectrum. It ranges from tiny stable nodules that may never cause problems, all the way through to disease that is already close to the point where radiotherapy becomes much less effective.
The key issue is not simply whether there is a lump in the hand. It is understanding what stage the disease has reached, whether there are signs of tightening already developing, and whether the hand is still within the stage where radiotherapy is most effective.
“It’s not affecting my hand function yet”
This is probably the most common thing patients say during a consultation. Many people assume that treatment is only necessary once the hand is clearly becoming difficult to use in daily life.
In reality, that is not how radiotherapy works. Radiotherapy is a preventative treatment. The aim is not to restore hand function once major functional loss has already developed. The aim is to stop the disease progressing to the point where significant contracture and functional limitation occur in the first place.
This is one reason many patients feel frustrated after seeing a General Practitioner (GP) or surgeon and being told, “Your fingers are still straight,” or “Come back when it gets worse.” Patients are often left feeling that nothing can be done until the disease has already progressed substantially, even though they can feel nodules, cords, tightness, or subtle changes beginning in the hand.
Historically, that approach made sense because surgery was the main treatment available, and surgery is designed to release established contractures. Radiotherapy changes the conversation because it works earlier in the disease process, before major contracture develops.
Why timing matters in Dupuytren’s disease
Radiotherapy and surgery are used at different stages of the disease because they do fundamentally different things.
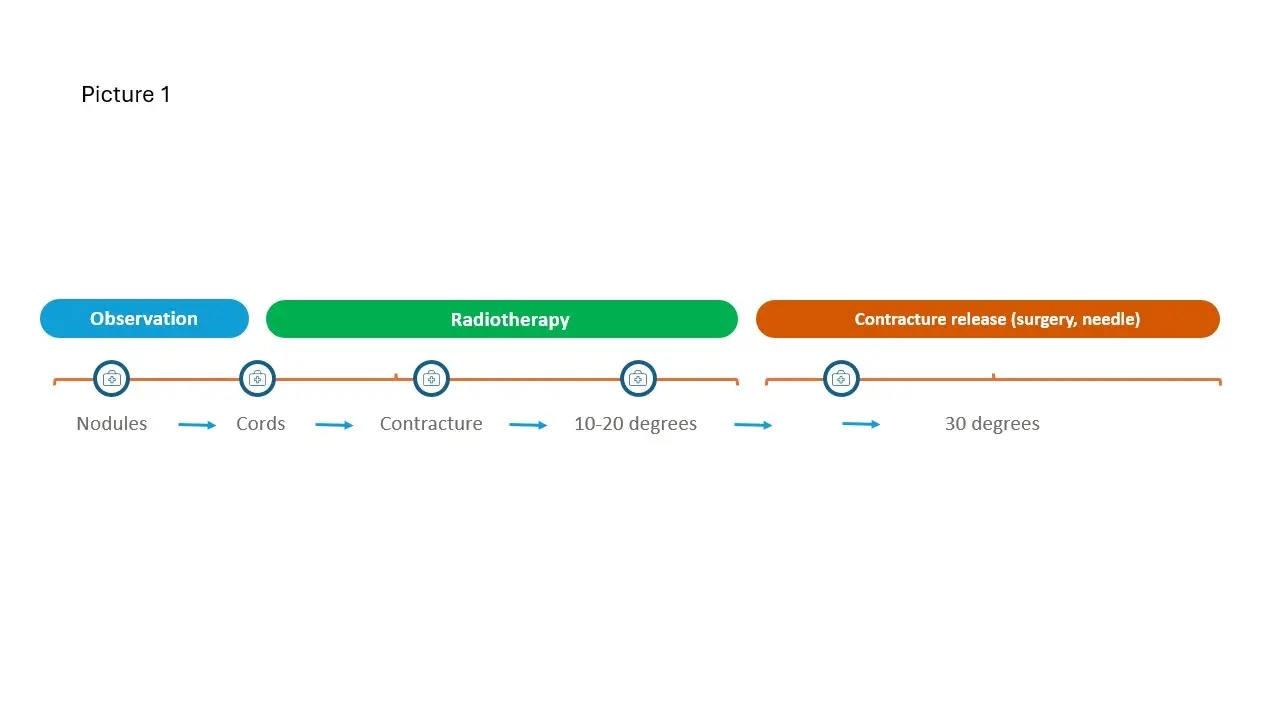
Surgery is most useful once a contracture has developed and the finger is physically being pulled into a bent position. Radiotherapy is most useful before an advanced contracture develops, ideally before there is any contracture at all. It can still sometimes be considered when there is a very mild contracture of around 10 to 20 degrees. Even at that stage, however, radiotherapy tends to be less effective than when the fingers are still fully straight.
This is one of the biggest misconceptions patients have when they first hear about radiotherapy. Many people understandably assume that radiotherapy should physically straighten a bent finger. In reality, radiotherapy is not designed to mechanically release tight cords. Instead, it works by reducing the activity of the cells responsible for producing the abnormal scar-like tissue that forms Dupuytren’s nodules and cords.
That is why the stage of disease matters so much. Radiotherapy is designed to stabilise active disease before major tightening develops. Surgery and needle procedures are designed to release contractures once they are already established.

So when is it too early?
Not every patient with a small nodule needs immediate treatment. Some very early nodules remain stable for years and never progress significantly, while others gradually become more active over time.
The important thing is not simply whether you can see or feel a lump. The important thing is understanding what stage the disease appears to be at and whether there are early signs that tightening is beginning.
This is why I increasingly talk about a “structured observation approach” rather than simply “watch and wait”. “Watch and wait” can sound passive, almost as though the patient is being told to ignore the condition until the finger bends badly enough to justify surgery. A structured observation approach is different. The aim is to properly assess the disease, understand whether there are signs of activity or tightening, and establish a clear plan for monitoring over time.
Importantly, this assessment needs to be done by someone experienced specifically in early Dupuytren’s disease. GPs are understandably not specialists in Dupuytren’s disease, and many hand surgeons mainly deal with later-stage contractures requiring surgery. Early Dupuytren’s disease is a very different clinical problem, because the key question is not how to release a contracture, but whether the hand is still within the optimal window for preventative treatment.
What are the signs that matter?
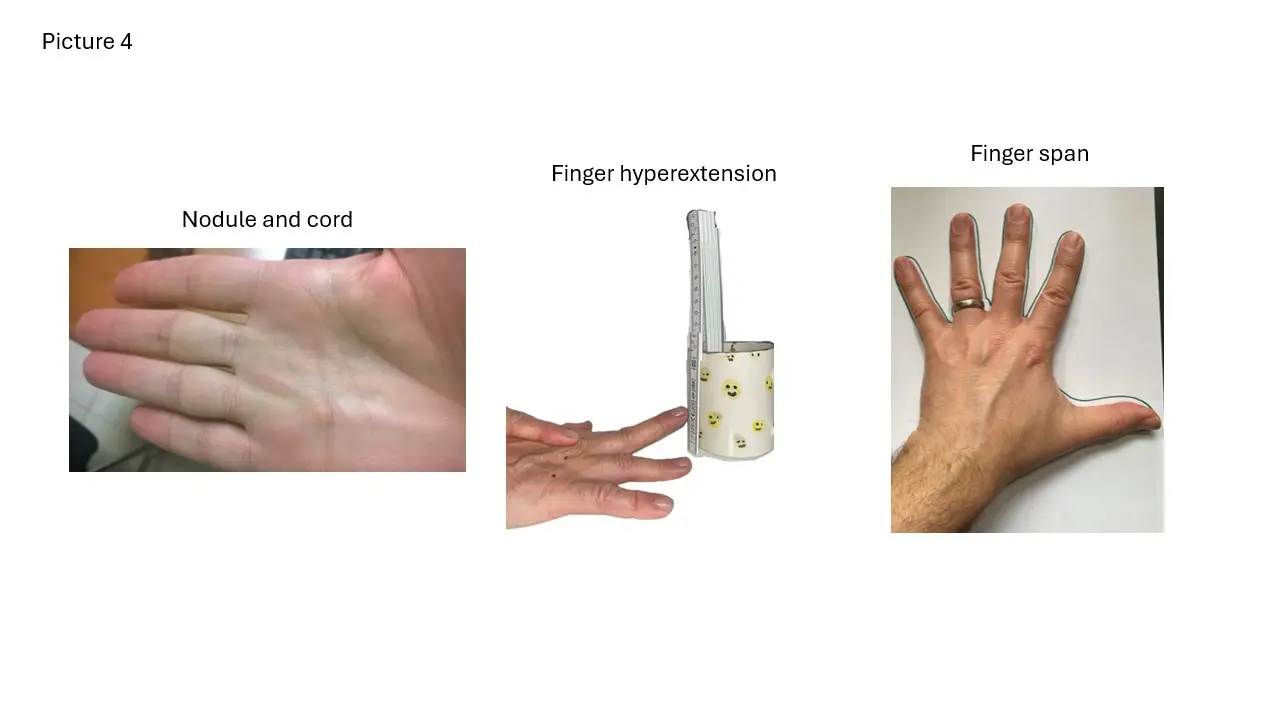
One important factor is the extent of disease in the hand. This includes the number and size of nodules, whether cords are forming, whether they are extending towards the fingers, and whether skin dimpling is developing.
Symptoms can also provide clues about disease activity. Some patients notice tenderness, itching, redness, or a sense that the hand feels tighter or more active. Others describe an increasing awareness of the cords or nodules, even if they cannot clearly explain why.
Subtle movement changes are often especially important. Many patients can still place their hand flat on a table and therefore assume there is no meaningful tightening. However, one of the earliest changes is often loss of hyperextension: in other words, reduced ability to bend the fingers backwards. This can occur before an obvious forward contracture develops.
Reduced finger span can also develop gradually. Patients sometimes notice increasing tightness between the fingers, or difficulty spreading the hand fully apart. These early movement changes can be clinically important even when patients are unsure whether the disease is “progressing” in the usual sense.
Why specialist assessment matters
One of the difficulties with Dupuytren’s disease is that gradual change can be surprisingly difficult for patients to judge themselves. If progression occurs slowly over months or years, many people adapt to the changes without fully realising how much movement has already been lost.
This is why specialist assessment is often valuable even when patients are unsure whether things are worsening. During a consultation, an expert in early Dupuytren’s disease can assess the pattern of nodules and cords, examine finger movement carefully, and look for early loss of hyperextension or finger span. This helps determine whether the hand appears to be moving towards the stage where radiotherapy is most useful.
In some cases, patients leave reassured that immediate treatment is not required. In others, assessment identifies early tightening or functional changes that patients themselves had not fully appreciated. Either way, patients usually leave with a much clearer understanding of what stage their disease has reached and what to look out for going forward.
Wondering what stage your hand is at?
If you have noticed nodules, cords or early tightening and are unsure whether the timing is right, a proper assessment can give you a clear answer. Get in touch with Dr Shaffer to find out what stage your hand is at and what your options are.

So, when is it too late?
Radiotherapy is most effective before advanced contracture develops. Once the fingers are significantly bent, the situation changes because the cords have physically shortened and tightened enough to pull the finger into a fixed position.
At that stage, the problem becomes mechanical and requires a mechanical solution. Patients with established contractures, therefore, generally need contracture-release procedures such as needle fasciotomy, collagenase injection where available, or surgical fasciectomy.
Patients often worry about whether they have already missed the opportunity for radiotherapy, but many people do not realise how difficult it can be to judge contracture severity accurately themselves. What one person describes as “a slight bend” may already represent substantial tightening, while another person may worry unnecessarily about very minor changes.
This is another reason why assessment by somebody experienced in early Dupuytren’s disease is so important. The decision is not based purely on whether a finger looks slightly bent to the patient. It depends on the overall stage of disease, the degree of contracture, the pattern of cords and nodules, and whether the hand still appears suitable for preventative treatment.
Most patients sit somewhere in the middle
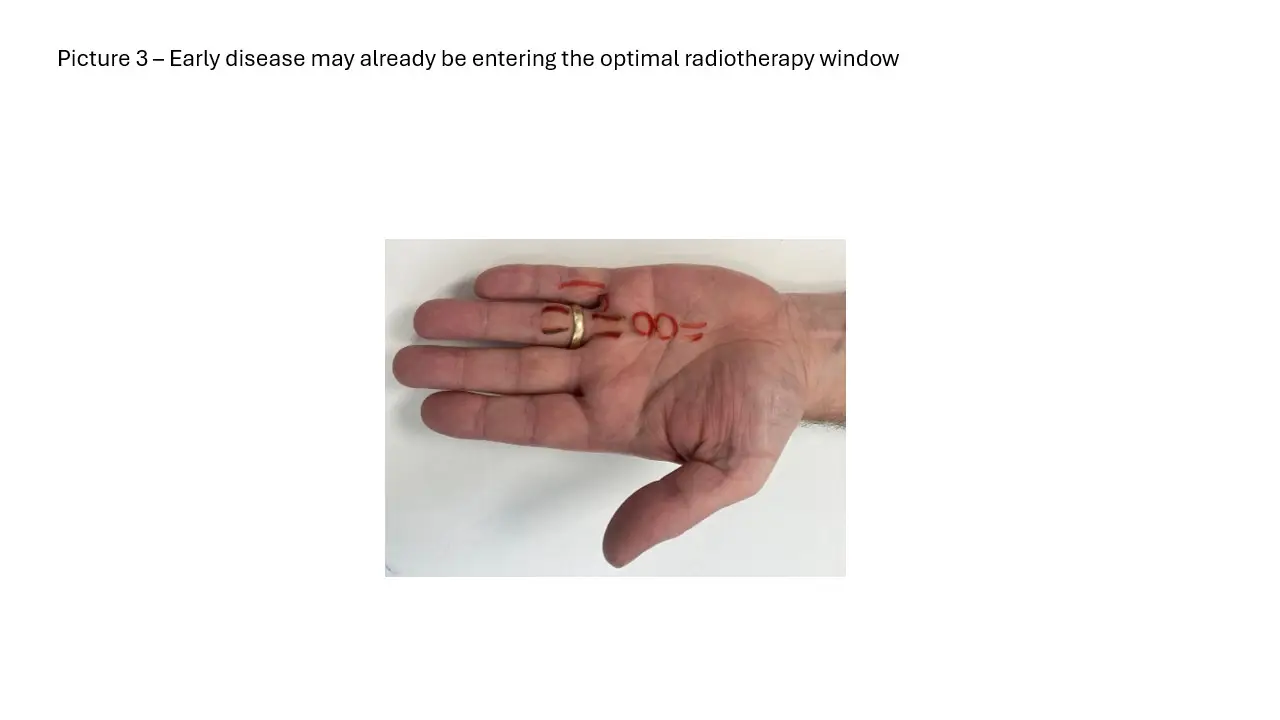
In reality, most people are not at either extreme. They are not simply sitting with one tiny stable lump, nor do they yet have severe contractures requiring surgery. Instead, many patients have enlarging nodules, developing cords, subtle loss of hyperextension, increasing tightness, or mild early contracture.
This middle stage is often where timing becomes most important and where specialist assessment becomes especially valuable. Patients are frequently told that their fingers are “not bad enough yet”, but at the same time may already be developing the very early tightening where radiotherapy is likely to work best.
The challenge is therefore not simply identifying “progression”. It is recognising when the disease is becoming established enough to justify preventative treatment while still remaining early enough for radiotherapy to be effective.
Are some patients more likely to need earlier treatment?
Some patients appear more prone to progression than others. Younger patients, those with strong family histories, people with disease affecting both hands, and patients developing cords relatively quickly may all be more likely to develop tightening over time.
Specialised hand use is also highly relevant. Musicians, surgeons, artists, and others who rely heavily on fine hand function often notice subtle changes much earlier than other patients. Small reductions in flexibility, span, or hyperextension may have a significant professional impact long before major contracture develops.
This does not necessarily mean such patients automatically need immediate treatment. However, it does make careful assessment and timing decisions particularly important.
The goal is not simply “treat early”
The goal is not to treat every tiny nodule immediately after it appears, but equally, it is not to wait until severe deformity develops before seeking specialist advice.
The real aim is to identify the stage where the disease is active enough to justify preventative treatment while still being early enough for radiotherapy to work effectively. Getting that timing right requires proper assessment by somebody experienced specifically in early Dupuytren’s disease.
Even if radiotherapy is not needed immediately, understanding what stage the disease has reached and having a structured plan for monitoring can make a major difference to long-term outcomes.
Final thoughts
If you have noticed nodules, cords, tightening, or subtle movement changes in your hand, it is worth getting properly assessed, even if your hand function still feels largely normal. Radiotherapy is a preventative treatment, which means the ideal stage for treatment is often before major functional loss develops.
Equally, if significant contracture has already developed, there are still effective treatment options available, although these are usually contracture-release procedures rather than radiotherapy.
The key is understanding what stage your disease is actually at and whether the hand still sits within the optimal window for preventative treatment. If you would like that assessed properly, you are welcome to get in touch.
References
NHS. Dupuytren’s contracture. Available at: nhs.uk/conditions/dupuytrens-contracture
British Society for Surgery of the Hand. Dupuytren’s disease. Available at: bssh.ac.uk/patients/conditions/25/dupuytrens_disease