If you’ve noticed a lump or cord in your palm and have spent the past few weeks quietly worrying, you are in good company.


“I feel like my future has changed overnight”
The emotional impact of a Dupuytren’s diagnosis often catches people off guard, particularly in those first weeks before they’ve had a chance to understand what it means.
Patients often describe being consumed by worry almost immediately after noticing the first signs. Thoughts quickly spiral towards the future. Will my fingers bend? Will I lose function? Will I still be able to work, exercise, play music, climb, paint, garden or use my dominant hand normally?
One patient online described constantly checking and stretching their fingers throughout the day, repeatedly asking: “Is it worse now?” Another talked about crying at night, mourning the future they thought they were going to have. Others described anger, bitterness, or a feeling that life had suddenly become unpredictable.
If you recognise yourself in those feelings, you are not unusual.
Why does a Dupuytren's diagnosis feel so frightening?
The anxiety is largely driven by uncertainty. Dupuytren’s disease behaves very differently from one person to the next. Some patients have a slow, mild course over many years. Others progress more quickly. This variability makes it natural to imagine the worst possible outcome. You can read more about how the condition typically develops on our symptoms and causes page.
The lack of a clear timeline can feel deeply unsettling. You may find yourself searching for certainty that nobody can give you, and that absence of certainty often gets filled with fear.
Did I cause this?
A very common reaction is trying to work out why this has happened.
Patients often blame manual work, the gym, typing, golf, climbing, vibration tools, previous injuries or overuse of the hand. In reality, Dupuytren’s disease is largely genetic. Research strongly suggests that most of the predisposition is inherited, according to NHS guidance on the condition [1].
There are associated factors, including smoking, alcohol intake, diabetes and certain metabolic conditions, but most patients did not cause their disease through something they personally did wrong.
That matters because self-blame quietly worsens the emotional burden.
The internet tends to show the worst cases
One of the recurring themes from patient discussions online is how frightening internet research can become. Many people arrive in the clinic convinced they are heading towards severe deformity because they have spent hours reading horror stories or looking at advanced cases.
There is an important bias in what you find online that most patients miss. People with mild, stable Dupuytren’s disease tend not to post about it. They simply get on with life. The voices you hear loudest are often those who have had complications, severe contractures or difficult surgical outcomes.
The full spectrum of Dupuytren’s disease is far broader. The typical experience is usually less dramatic than the most alarming stories suggest.
What do patients say further down the road?
Early days are often the hardest. Many patients describe how life gradually returned to normal. You can read real experiences on our patient case studies page. Common reflections from those further along include:
“It’s not nearly as bad as I feared in those first weeks.”
“I’m still working with my hands.”
“I’m still doing almost everything I used to do.”
“It just became one part of life rather than the centre of everything.”
That does not mean dismissing the disease or pretending it is insignificant. The shock of those first weeks almost always fades. Most patients look back and say the fear was worse than the reality.
Getting clarity: what a proper assessment actually involves
Many patients feel frustrated because they are simply told to “come back when the fingers bend.” While monitoring is often appropriate, that advice can leave people feeling powerless. In our experience, the patients who struggle most with Dupuytren’s anxiety are those given no clear markers to watch for. That passive uncertainty is avoidable.
One of the most important shifts is moving away from helpless uncertainty towards informed understanding. That does not necessarily mean rushing into treatment. It means properly understanding where you are on the spectrum of disease. Our overview of Dupuytren’s disease explains the full picture.
This is where seeing someone with particular expertise in Dupuytren’s disease becomes valuable. A proper assessment is not simply about confirming the diagnosis. It is about understanding your individual pattern, your risk of progression, and the realistic range of options available to you, both now and in the future. You can book a consultation with Dr Richard Shaffer at any stage.
Expert Non-Invasive Treatment for Dupuytren’s and Ledderhose Disease Across the UK
Dr Richard Shaffer set up Dupuytren’s UK in April 2011 to provide non-invasive treatments for people who suffer from benign conditions such as Ledderhose disease and early-stage Dupuytren’s contracture in the Guildford area. Today, Dupuytren’s UK offers this service to patients throughout the UK.

What options are available?
Much of the panic in early Dupuytren’s disease comes from feeling like nothing can be done. Once patients understand there are different approaches at different stages, the fear usually softens.
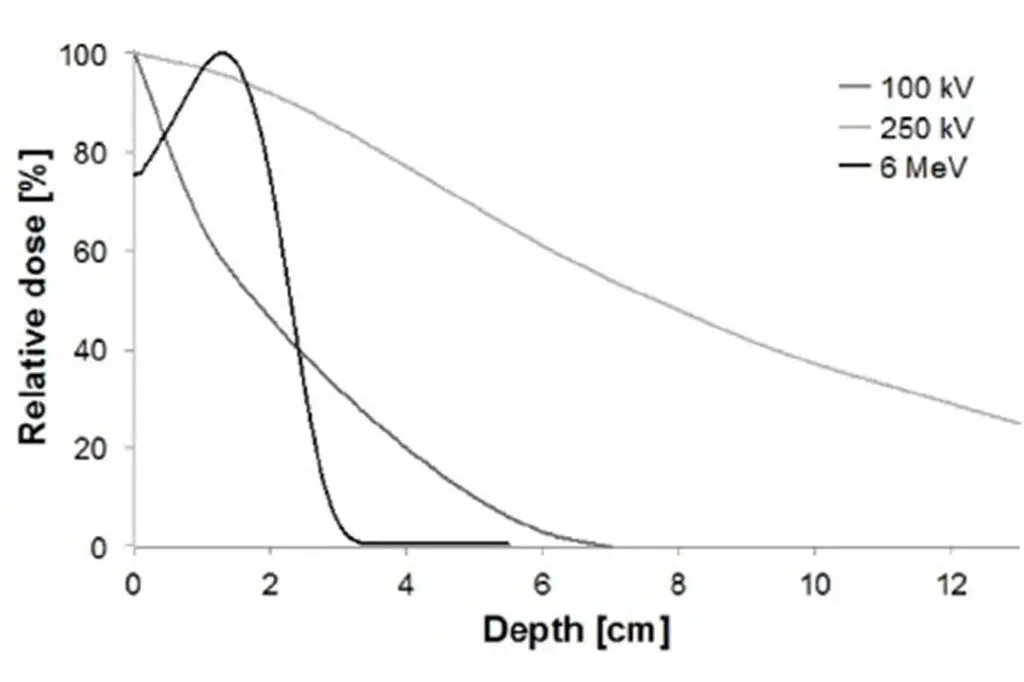
Depending on where you are on the spectrum, options range from careful monitoring and lifestyle adjustments to low-dose radiotherapy (a short course of targeted X-ray treatment) in earlier stages. If a contracture has developed, surgical or needle-based procedures may also be discussed. Your specialist will explain which options are realistic for your situation and what the evidence says about each. Our diagnosis and treatments page covers all the options in detail.
Learning about the early-stage option of low-dose radiotherapy for Dupuytren’s disease, which may be suitable for some patients before a significant contracture has set in, can give a clearer picture of what is available to you.
Build a plan, not a panic response
A plan does not have to mean treatment. For some patients, it simply means scheduled reviews, photographs of the hand, and clear markers to look out for, such as new cords, increasing thickness, or any difficulty placing the palm flat on a table (the tabletop test, where you press your palm downwards and observe whether your fingers lie flat).
For others, it may mean exploring earlier treatment options before a contracture develops.
The key is moving from passive worry to active monitoring, so you know what is changing over time. Having a sensible plan changes the emotional experience completely. Instead of feeling trapped waiting for something terrible to happen, you start to feel informed and in control.
Will I still be able to live normally?
One of the strongest themes from real patient experiences is that many people continue working, exercising, and doing most of what they did before their diagnosis.
Patients online have described continuing to work with their hands, raising families, running, painting and even playing string instruments years after diagnosis. Some make small adjustments. Others focus more carefully on overall health and well-being. The diagnosis itself does not mean life suddenly stops.
Several patients also spoke about practical ways they improved their mental resilience: exercise, focusing on general health, therapy aimed at coping with chronic illness, gratitude journaling, and reducing constant checking behaviours.
Living well psychologically matters just as much as monitoring the physical condition itself. If your low mood, anxiety or sleep is significantly affected, speaking to your GP is a good idea. They can advise on local mental health support.
The next steps: getting proper guidance
The most helpful next step is usually twofold.
First, try to shift your thinking away from catastrophic future scenarios and back towards the reality of your current situation. Not every nodule (a small, firm lump under the skin) progresses rapidly. Not every patient develops a severe contracture. The goal is not to spend years mentally living in a future that may never happen. Our page on symptoms and causes of Dupuytren’s disease can help you understand what to watch for.
Second, get clarity from someone experienced in Dupuytren’s disease. Understanding exactly where you are on the spectrum, whether there are signs of progression, and what your realistic options are at this stage can make an enormous difference, psychologically as well as medically. You can find out more about Dr Richard Shaffer and his approach before booking.
For some patients, that process provides reassurance that monitoring is the right approach. For others, it may identify that early treatment options should be discussed before a more significant contracture develops. Understanding your own situation properly is almost always better than facing the uncertainty alone.
Frequently asked questions
Does Dupuytren's disease always get worse?
No. Dupuytren’s disease is unpredictable, and many patients have a slow or very mild course over many years. Some people notice little change for decades. Regular monitoring helps identify whether and how quickly your condition is progressing, which informs the most appropriate approach. See the NHS overview for further information [1].
What is the tabletop test?
The tabletop test is a simple self-check: place your hand palm-down on a flat surface and observe whether all your fingers lie flat. If one or more fingers cannot fully flatten, it may suggest the beginning of a contracture.
Can stress or anxiety make Dupuytren's disease worse?
There is no established clinical evidence that psychological stress accelerates Dupuytren’s progression. However, anxiety can make living with the condition significantly harder. Addressing your mental well-being is a worthwhile part of managing any long-term condition.
When should I see a specialist?
If you have noticed a new lump, cord, or any change in finger movement, or if you simply want clarity on where you stand, it is worth arranging a specialist assessment. You do not need to wait until your fingers have begun to bend. Earlier assessment often means more options available to you. You can book a consultation here.
Is Dupuytren's disease genetic?
Yes, Dupuytren’s disease has a strong genetic component. It runs in families and is particularly common in people of Northern European descent. Having a close family member with the condition increases your likelihood of developing it, though not everyone with a family history will be affected.
Related reading on Dupuytren's UK
If you would like to learn more about the condition itself, our pages on Dupuytren’s disease, symptoms and causes of Dupuytren’s, and case studies from other patients may be useful. If you are ready to discuss your situation with a specialist, you can book an appointment with Dr Richard Shaffer or send an enquiry through our consultation page.